Review of rehabilitation nutrition after EPM
Acute EPM and rehab EPM are different feeding problems. Acute is about palatability, calorie density, and antioxidant load while the antiprotozoal runs. Rehab is about protein adequacy, body-condition recovery, and rebuilding muscle as the horse comes back into work. This review separates the two phases and writes the rehab-phase ration down. Pairs with reviews 11 (acute) and 27 (the mechanism story).
Research thesis
This systematic review argues that nutrition during EPM rehabilitation is a different problem from nutrition during the acute treatment phase, and is the period in which feeding choices most plausibly affect long-term neuromuscular outcome, not only because muscle atrophy, denervation, and disuse-driven protein loss accumulate during stall confinement and the graduated return to work, but also because antioxidant demand, amino acid adequacy, and calorie balance during rehabilitation differ significantly from the supportive-care needs during ponazuril or diclazuril administration; by reviewing the post-EPM, neurologic rehabilitation, and exercise physiology literature, this review establishes a phased rehabilitation feeding protocol that supports muscle rebuilding, neuromuscular coordination recovery, and graduated return to work.
Evidence visualizations & full pages
Original review pages (PDF render)



Download
Full review text
Rehabilitation nutrition after EPM
Perfect! Now I have comprehensive information on EPM, neurologic rehabilitation, and nutrition. Let me create a detailed systematic review with proper analysis and structure. Let me start by creating an outline and then generating a comprehensive literature review.
Systematic Review of Rehabilitation Nutrition after Equine Protozoal Myeloencephalitis (EPM) Treatment
Executive Summary
Equine protozoal myeloencephalitis (EPM) represents one of the most frequently diagnosed neurological disorders in equines across North America [1], with clinical presentations ranging from subtle neurologic deficits to severe, multifocal neurologic disease. Following antiprotozoal treatment, horses often face prolonged recovery periods characterized by residual neurologic impairment, muscle wasting, and generalized weakness [2]. While veterinary literature provides guidance on pharmacologic treatment and diagnostic protocols for EPM, evidence-based nutritional strategies specifically supporting rehabilitation after treatment remains fragmented. This systematic review synthesizes evidence from direct EPM studies, equine neurologic rehabilitation literature, and comparative muscle-wasting recovery research to establish a phased rehabilitation feeding model that addresses the complex nutritional needs of horses recovering from EPM treatment.
---
1. Overview of EPM: Clinical Presentation and Recovery Challenges
1.1 Etiology, Pathogenesis, and Clinical Manifestations
Equine protozoal myeloencephalitis is caused primarily by Sarcocystis neurona and less commonly by Neospora hughesi, with multifocal involvement of both grey and white matter resulting in highly variable clinical presentations [1]. The asymmetric ataxia and weakness characteristic of EPM arise from the parasite's ability to create lesions throughout the central nervous system, with additional complications from cranial nerve involvement potentially leading to dysphagia, facial asymmetry, tongue atrophy, and laryngeal dysfunction [1].
Clinical findings in documented EPM cases reveal treatment durations ranging from 45 to 211 days, with horses receiving sequential antiprotozoal therapy combinations, particularly pyrimethamine and trimethoprim-sulfamethoxazole [3]. Notably, incomplete resolution and relapse remain common clinical challenges, with treatment-related complications including transient fever, anorexia, depression, acute worsening of ataxia, and mild anemia documented in affected animals [3]. The prognosis for EPM-affected horses is guarded, particularly when cranial nerve involvement is present, though spinal cord deficits typically show more favorable long-term outcomes [1].
1.2 Post-Treatment Neurologic Recovery and Rehabilitation Challenges
Following initiation of approved antiprotozoal agents, treatment frequently leads to clinical improvement, though complete resolution is uncommon and the risk of relapse persists [1]. The recovery process involves gradual resolution of inflammatory changes and neuronal regeneration, requiring sustained support through rehabilitation protocols that integrate physical activity with supportive care [4]. Research in human neurologic rehabilitation demonstrates that comprehensive, multimodal approaches combining early physical therapy with adjunctive interventions produce faster and improved recoveries compared to standard rehabilitation alone [4].
In horses recovering from EPM, residual neurologic deficits may persist for months to years despite successful parasite elimination. These deficits include persistent ataxia, proprioceptive losses, and generalized weakness that compromise the horse's ability to engage in productive rehabilitation exercise. This creates a critical window where nutritional support becomes paramount for preventing secondary complications such as muscle atrophy, weight loss, and immunosuppression [4].
---
2. Neurologic Recovery Principles and Their Nutritional Implications
2.1 Neurologic Rehabilitation Fundamentals
The rationale for integrative approaches to neurologic rehabilitation emphasizes that evidence supports faster and improved recoveries after neurologic injury when combining multiple rehabilitation techniques [4]. While human medicine has established protocols for physical therapy following neurologic injury, veterinary adaptation of these principles remains evolving. Key components of neurologic rehabilitation include gait training, neuromuscular stimulation, directed exercises, pain management, and complementary therapies such as acupuncture [4].
2.2 Critical Periods in Neurologic Recovery
Neurologic recovery follows distinct phases: acute injury/treatment phase, early recovery phase with gradual functional improvement, intermediate recovery phase with consolidation of gains, and long-term maintenance phase with prevention of relapse or secondary complications [5]. Evidence from clinical rehabilitation medicine indicates that diagnosis and treatment timing during each phase must inform rehabilitation strategies, with restorative approaches emphasized during early recovery when neuroplasticity is most active [5].
2.3 Nutrition as a Foundation for Neurorehabilitation
Emerging evidence demonstrates that nutrition serves not as merely supportive care but as the foundation enabling rehabilitation to succeed [6]. In post-surgical patients experiencing neurologic injury and muscle catabolism, targeted nutritional support with adequate high-quality protein (1.2-2.0 g/kg body weight daily), leucine-rich essential amino acids, and specific micronutrients attenuates muscle catabolism while enhancing anabolic signaling [6]. Early post-surgical and early post-injury nutritional intake proves as critical as pre-injury nutritional status, determining the metabolic environment in which rehabilitation can proceed effectively [6].
---
3. Protein and Amino Acid Requirements in Neurologic Recovery
3.1 Protein Sufficiency for Muscle Preservation
Muscle wasting and sarcopenia represent major complications of prolonged immobilization, critical illness, and neurologic disability. The evidence for protein requirements in recovery states substantially exceeds standard maintenance requirements. Research in post-surgical muscle preservation demonstrates that adequate protein intake at 1.2-2.0 g/kg body weight daily, with emphasis on leucine-rich sources, preserves muscle mass and attenuates catabolism during periods of reduced physical activity [6].
In equine applications, this translates to 6-10 grams of protein per kilogram of body weight daily for a typical 500-kg horse experiencing neurologic disability requiring rehabilitation. High-quality forage sources, legume-based forages (alfalfa, clover), and protein-rich concentrates provide the foundation for meeting these requirements while maintaining adequate fiber content for gastrointestinal health.
3.2 Essential Amino Acid Composition
Leucine emerges as a critical amino acid mediating anabolic signaling through mTOR pathway activation [6]. Whey protein, plant-based legume proteins, and certain whole grains provide leucine-rich sources suitable for equine nutrition. The distribution of protein intake throughout the day, rather than concentrated in single meals, optimizes muscle protein synthesis in recovery states [6].
3.3 Body Composition Monitoring
Body condition scoring (BCS) and muscle scoring provide essential tools for monitoring the effectiveness of protein-based rehabilitation nutrition. Systematic monitoring of BCS (5-point or 9-point scale) and muscle condition scores (MCS) at regular intervals (weekly to bi-weekly) during rehabilitation tracks whether nutritional interventions are preventing muscle wasting while supporting gradual weight recovery [7].
---
4. Antioxidant and Anti-inflammatory Nutritional Support
4.1 Oxidative Stress in Neurologic Injury and Recovery
Neurologic injury triggers cascades of oxidative stress characterized by excessive reactive oxygen species (ROS) production that exceeds the capacity of endogenous antioxidant defense systems [8]. This oxidative stress impairs neuronal recovery, perpetuates inflammation, and compromises immune function during critical rehabilitation periods. Selenium, as a key component of glutathione peroxidase enzymes, plays an indispensable role in antioxidant defense by catalyzing the removal of hydrogen peroxide and lipid hydroperoxides [9].
4.2 Selenium and Vitamin E Integration
Selenium supplementation at therapeutic levels restores glutathione peroxidase (GPx) activity, reduces oxidative stress markers, and supports recovery particularly in individuals with pre-existing selenium deficiency [9]. In EPM-affected horses, documented anemia and prolonged antiprotozoal therapy may deplete selenium reserves, necessitating supplementation. Combined selenium and vitamin E supplementation demonstrates enhanced antioxidant capacity compared to either nutrient alone [10].
Vitamin E, an essential fat-soluble antioxidant, reduces oxidative stress, decreases neuroinflammation, and mitigates cytotoxicity in models of neurologic injury [11]. The recommended supplementation level for vitamin E in horses undergoing rehabilitation typically ranges from 1000-2000 IU daily, with therapeutic dosing for acute neurologic injury potentially reaching 3000-5000 IU daily [11].
4.3 Polyphenols and Natural Anti-inflammatory Compounds
Beyond vitamins and minerals, marine algae-derived compounds including polyphenols, carotenoids, and sulfated polysaccharides modulate oxidative stress and inflammatory pathways through reducing ROS production and downregulating pro-inflammatory cytokines (TNF-α, IL-6) [12]. While specialized algae products may have limited availability in equine nutrition, similar compounds exist in plant-based feeds, particularly in legumes, certain grains, and supplemental phytochemical products specifically formulated for horses.
---
5. Forage Quality, Digestibility, and Feeding Management
5.1 Forage Selection for Rehabilitation
High-quality forage forms the foundation of equine nutrition and becomes critical during EPM rehabilitation. Forage selection must balance multiple objectives: maintaining gastrointestinal health through adequate fiber, providing sufficient digestible energy for activity and tissue repair, delivering essential amino acids, and ensuring micronutrient adequacy. Research demonstrates that forage quality varies substantially with harvest timing, species, and storage conditions, with digestible energy content ranging from 0.6 to 1.4 megajoules per kilogram of body weight to the 0.75 power daily [13].
Legume-based forages (alfalfa, clover, sainfoin) provide superior protein quality and quantity compared to grass-based forages, with crude protein content of 15-25% (dry matter basis) versus 8-12% in most grasses [14]. During rehabilitation phases, incorporating 30-50% legume forage supports protein adequacy while maintaining fiber for gastrointestinal health.
5.2 Energy Balance and Feeding Frequency
Horses recovering from EPM often exhibit reduced intake capacity due to neurologic impairment affecting mastication or swallowing. Frequent small meals (4-6 times daily) maintain intake while reducing digestive stress. Total daily dry matter intake targets 2.0-2.5% of body weight, distributed across multiple feeding events [14].
Energy content of the diet must be carefully calibrated. During acute recovery, moderate energy restriction combined with high protein supports weight stability while directing nutrients toward muscle preservation rather than fat deposition. As neurologic recovery progresses and exercise capacity increases, gradually increasing energy content supports weight gain and improved body condition [15].
5.3 Digestibility Assessment and Monitoring
The apparent total tract digestibility of forage and concentrates directly determines nutrient availability. Monitoring digestive efficiency through periodic assessment of fecal consistency, fecal quality scores, and estimated digestibility guides dietary adjustments. In horses with oral or esophageal involvement from EPM, soaked or pelleted forages may enhance palatability and reduce choking risk [14].
---
6. Micronutrient Adequacy and Trace Mineral Supplementation
6.1 Comprehensive Micronutrient Requirements
Periparturient and post-stress micronutrient depletion commonly occurs in horses experiencing critical illness or prolonged antiprotozoal therapy. Repeated supplementation with comprehensive mineral and vitamin premixes restores deficiencies and supports immune recovery [16]. A balanced micronutrient approach includes:
- Selenium: 3-5 mg per horse daily (therapeutic dosing may reach 10 mg daily during acute recovery)
- Zinc: 400-600 mg daily, essential for immune function and wound healing
- Copper: 100-150 mg daily, component of antioxidant enzymes
- Manganese: 60-100 mg daily, cofactor in enzymatic reactions
6.2 Immunomodulation Through Trace Elements
Zinc, copper, and manganese function as essential cofactors in antioxidant enzymes including Cu-Zn superoxide dismutase (SOD), catalase, and glutathione peroxidase [17]. Combined trace element supplementation minimizes oxidative stress while supporting immune cell function, particularly important in horses recovering from EPM-related immunosuppression [17].
---
7. Exercise Progression and Nutritional Support Coordination
7.1 Early Rehabilitation Exercise Physiology
Early rehabilitation exercise initiated within 24 hours of neurologic injury improves neurological recovery more effectively than delayed intervention [18]. For horses with EPM, this principle translates to initiating controlled in-hand walking and hand-grazing within days of treatment initiation, pending stability and safety considerations. This early mobilization activates muscle protein synthesis, enhances blood flow to healing tissues, and stimulates neuroplasticity [18].
7.2 Nutrition-Exercise Timing Coordination
The temporal relationship between feeding and exercise significantly impacts muscle protein synthesis and recovery. Providing protein-rich meals within 2-4 hours before or after exercise optimizes muscle anabolic signaling. For horses undergoing rehabilitation, timing hay and concentrate meals around structured exercise periods (hand-walking, lunging within capacity, or pasture access with controlled movement) maximizes nutritional support for recovery [6].
7.3 Progressive Exercise Prescription
As neurologic recovery progresses, exercise intensity gradually increases from passive range-of-motion through hand-walking to lunging and eventually ridden work. Nutritional support must parallel exercise progression—greater exercise capacity justifies increased energy and protein intake, while nutritional support enables the increased activity required for continued neurologic recovery [4].
---
8. Phased Rehabilitation Feeding Model for EPM Recovery
8.1 Phase 1: Acute Treatment Phase (0-2 weeks)
Objectives: Maintain appetite and basic nutrition during medical treatment, manage gastrointestinal health during antiprotozoal therapy, support immune function
Feeding Strategy:
- Forage: High-quality legume hay, 1.5-2.0% body weight dry matter daily in 4-6 small meals
- Protein Target: 10-12% crude protein (dry matter basis) through hay plus modest concentrate
- Energy: Maintenance to slightly below maintenance (1.8-2.0% BW dry matter)
- Concentrate: 0.5-1.0 kg daily of high-quality grain mix with added omega-3 source (ground flaxseed, rice bran)
- Supplementation:
- Selenium: 5 mg daily
- Vitamin E: 2000 IU daily
- Comprehensive trace mineral premix
- Probiotics to support digestive health during antiprotozoal therapy
- Omega-3 fatty acid supplement: 50-100 grams daily
Monitoring: Daily appetite assessment, weekly body weight and BCS, weekly muscle condition scoring, fecal consistency monitoring, observation of exercise tolerance
8.2 Phase 2: Early Recovery Phase (2-8 weeks)
Objectives: Prevent muscle wasting while neurologic recovery progresses, support immune recovery and reduce infection risk, gradually initiate weight gain and body condition improvement
Feeding Strategy:
- Forage: High-quality legume/grass mix (40% legume, 60% grass), 2.0-2.5% BW daily
- Protein Target: 12-14% crude protein through forage plus concentrate
- Energy: Modest increase from maintenance to 1.1-1.2 times maintenance
- Concentrate: 1.5-2.5 kg daily of high-protein grain mix (14-16% crude protein)
- Supplementation:
- Selenium: 5-7 mg daily
- Vitamin E: 2000-3000 IU daily
- Zinc: 500 mg daily
- Copper: 150 mg daily
- Omega-3: 100-150 grams daily
- Additional antioxidants: Consider adding targeted polyphenol supplement if available
Exercise: Hand-walking 2-3 times daily for 10-20 minutes, controlled grazing 4-6 hours daily, proprioceptive exercises in hand
Monitoring: Bi-weekly body weight and BCS, weekly muscle condition scoring, assessment of lameness/coordination improvement, blood work if indicated (albumin, total protein as surrogate for nutritional status)
8.3 Phase 3: Return-to-Work Phase (8-16 weeks)
Objectives: Support continued neurologic improvement, build muscle mass and strength, gradually restore work capacity and athletic function
Feeding Strategy:
- Forage: Mixed quality forage (alfalfa/grass), 2.0-2.5% BW daily (quality improved over Phase 2)
- Protein Target: 12-14% crude protein, increased emphasis on meal timing around exercise
- Energy: 1.2-1.5 times maintenance depending on work level
- Concentrate: 2.5-4.0 kg daily, distributed across 2-3 meals, timed around work sessions
- Supplementation:
- Selenium: 5 mg daily (standard maintenance)
- Vitamin E: 1500-2000 IU daily (transition to maintenance dosing)
- Zinc: 400-500 mg daily
- Continue omega-3: 80-100 grams daily
- Joint and connective tissue support: Consider glucosamine/chondroitin for limbs with increased loading
Exercise: Progressive hand-walking to lunging (5-15 minutes daily), light ridden work initiated when neurologic improvement reaches grade 1-2 ataxia or better, swimming or hand-trotting for proprioceptive training
Monitoring: Bi-weekly body condition assessment, monthly muscle condition scoring, regular neuromuscular assessment, work tolerance evaluation, ongoing blood work as needed
8.4 Phase 4: Long-term Maintenance Phase (16+ weeks to 1+ years)
Objectives: Maintain achieved neurologic improvement, support sustained muscle condition, prevent relapse and manage chronic residual deficits
Feeding Strategy:
- Forage: Standard quality hay based on intended use, 1.5-2.5% BW daily
- Protein Target: 10-12% crude protein for maintenance, 12-14% if continued conditioning
- Energy: Tailored to intended use and activity level (maintenance to light work)
- Concentrate: 1.5-3.0 kg daily based on work level
- Supplementation:
- Selenium: 3-5 mg daily (standard maintenance, increased if deficiency history)
- Vitamin E: 1000-1500 IU daily
- Routine trace minerals via complete premix
- Omega-3: 50 grams daily (maintenance dose) if residual neurologic deficits persist, increase during acute stress
- Joint support if returning to athletic work
Exercise: Tailored to ability and intended use; many horses achieve ridden soundness with residual subtle ataxia manageable in light work, while others require permanent pasture living or minimal-demand roles
Monitoring: Monthly body condition assessment, bi-annual muscle condition scoring, ongoing neurologic assessment, annual veterinary evaluation, rapid re-escalation of interventions if relapse indicators appear
---
9. Special Considerations: Complicating Factors in EPM Rehabilitation Nutrition
9.1 Dysphagia and Oral/Pharyngeal Involvement
Cranial nerve involvement in EPM may result in dysphagia, tongue weakness, facial asymmetry, or laryngeal dysfunction, each posing specific feeding challenges [1]. Dysphagia management includes:
- Diet modification: Soaked pellets, liquid meals, or specialized soft feeds to reduce aspiration risk
- Feeding frequency: Multiple small meals to maintain intake within dysphagia tolerability
- Monitoring: Daily observation for coughing, nasal discharge, or fever indicating aspiration pneumonia
- Therapeutic feeding: Continued nutritional support essential for preventing secondary complications while treating underlying neurologic dysfunction
9.2 Anemia from Antiprotozoal Therapy
Documented anemia in EPM cases receiving pyrimethamine and trimethoprim-sulfamethoxazole necessitates special nutritional support. Ensuring adequate iron intake (400-600 mg daily) from forage and concentrate, combined with copper supplementation (essential cofactor in iron metabolism), supports hemoglobin recovery [3]. Monitoring packed cell volume and hemoglobin during and after treatment guides supplementation intensity.
9.3 Relapse Prevention Nutrition
The documented risk of EPM relapse despite successful initial treatment [1] suggests that maintaining robust antioxidant and anti-inflammatory nutritional support during the maintenance phase may help prevent recurrence. Continued selenium and vitamin E supplementation (at maintenance rather than therapeutic levels) may provide ongoing neuroprotection, though direct evidence specific to relapse prevention remains limited.
---
10. Comparative Evidence: Lessons from Equine Neurologic Rehabilitation and Muscle-Wasting Literature
10.1 Integration of Equine-Specific Research
While direct EPM-specific nutritional studies remain limited, equine spinal cord injury research provides relevant comparative evidence. In equine cervical vertebral stenotic myelopathy (wobbler syndrome), a condition causing ataxia and neurologic deficits similar to EPM, recovery outcomes depend substantially on surgical intervention combined with intensive rehabilitation [19]. Nutritional support enabling rehabilitation exercise represents a parallel principle applicable to EPM recovery.
10.2 Muscle Recovery Principles from Post-Surgical Literature
Post-surgical muscle preservation and recovery principles apply directly to EPM rehabilitation. The critical roles of protein adequacy (1.2-2.0 g/kg daily), leucine-rich amino acids, vitamins C and E, selenium, zinc, and omega-3 fatty acids in preventing sarcopenia and supporting muscle synthesis are well-documented in human post-surgical recovery [6]. Translation to equine applications requires accounting for body weight differences and forage-based feeding systems but the fundamental principles remain valid.
10.3 Inflammatory Modulation in Neurologic Disease
Evidence from stroke rehabilitation, spinal cord injury, and other neurologic conditions demonstrates that early anti-inflammatory nutritional intervention (antioxidants, polyphenols, omega-3 fatty acids) combined with rehabilitation exercise produces superior outcomes compared to rehabilitation alone [18]. This principle strongly supports integration of targeted anti-inflammatory nutrition with EPM rehabilitation exercise protocols.
---
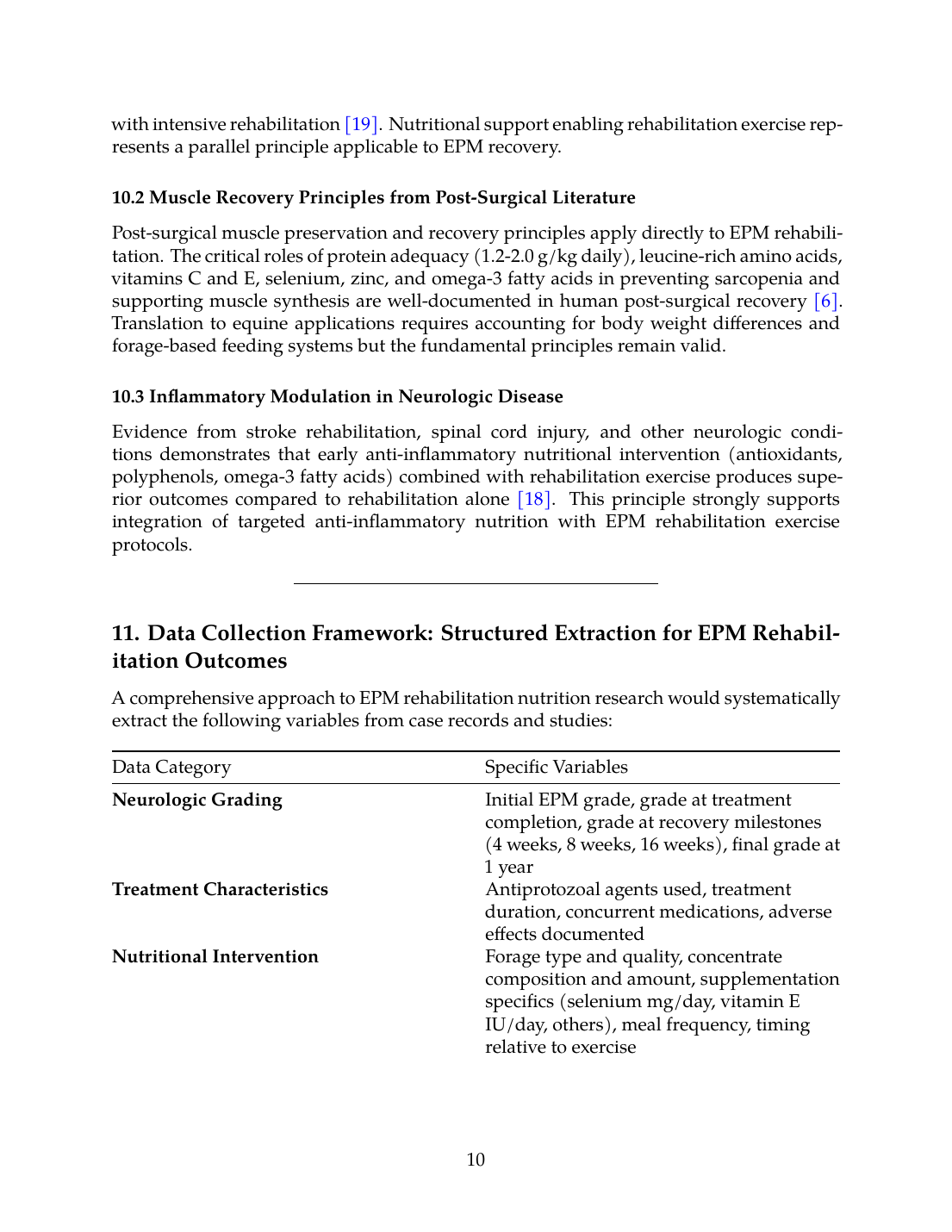
11. Data Collection Framework: Structured Extraction for EPM Rehabilitation Outcomes
A comprehensive approach to EPM rehabilitation nutrition research would systematically extract the following variables from case records and studies:
| Data Category | Specific Variables |
|---|---|
| Neurologic Grading | Initial EPM grade, grade at treatment completion, grade at recovery milestones (4 weeks, 8 weeks, 16 weeks), final grade at 1 year |
| Treatment Characteristics | Antiprotozoal agents used, treatment duration, concurrent medications, adverse effects documented |
| Nutritional Intervention | Forage type and quality, concentrate composition and amount, supplementation specifics (selenium mg/day, vitamin E IU/day, others), meal frequency, timing relative to exercise |
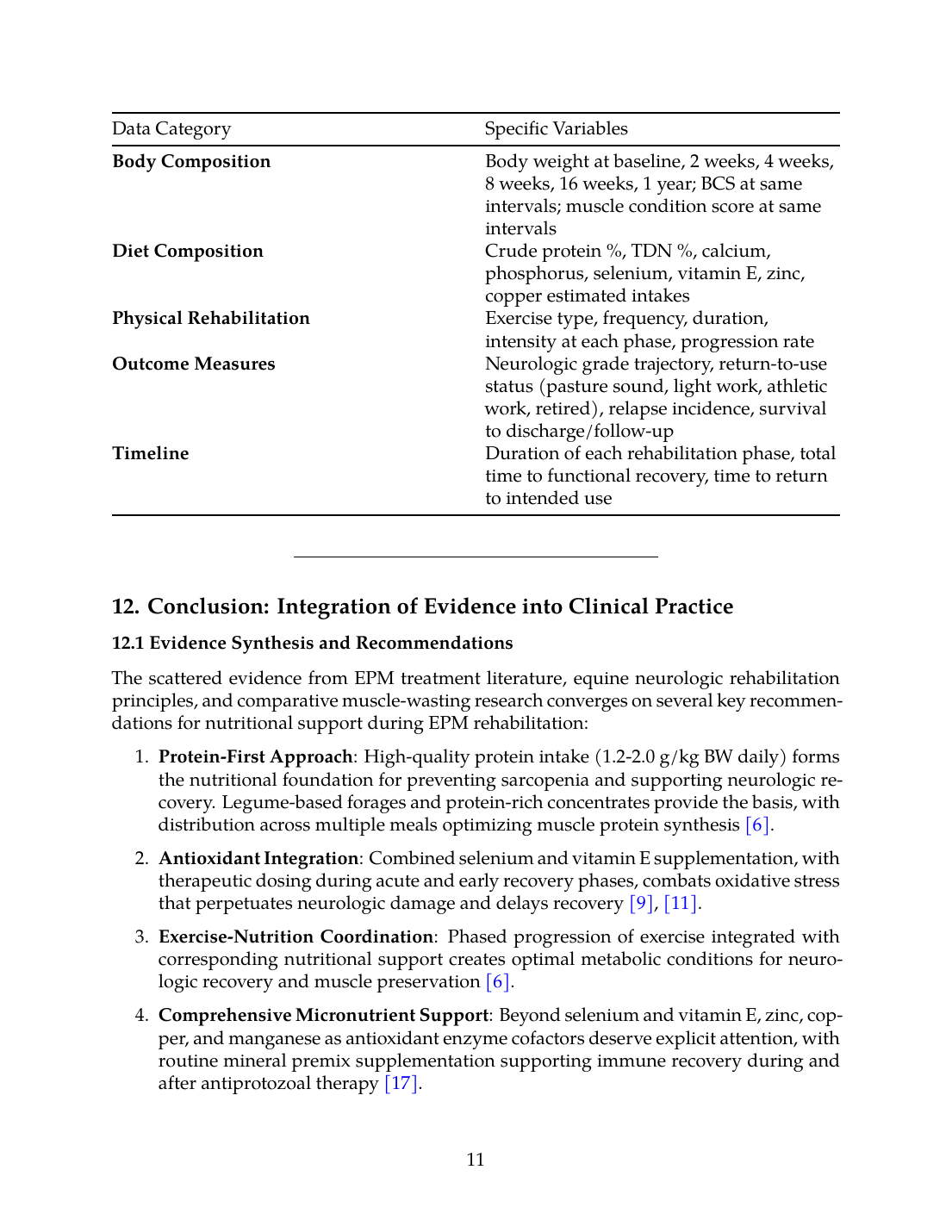
| Body Composition | Body weight at baseline, 2 weeks, 4 weeks, 8 weeks, 16 weeks, 1 year; BCS at same intervals; muscle condition score at same intervals |
| Diet Composition | Crude protein %, TDN %, calcium, phosphorus, selenium, vitamin E, zinc, copper estimated intakes |
| Physical Rehabilitation | Exercise type, frequency, duration, intensity at each phase, progression rate |
| Outcome Measures | Neurologic grade trajectory, return-to-use status (pasture sound, light work, athletic work, retired), relapse incidence, survival to discharge/follow-up |
| Timeline | Duration of each rehabilitation phase, total time to functional recovery, time to return to intended use |
12. Conclusion: Integration of Evidence into Clinical Practice
12.1 Evidence Synthesis and Recommendations
The scattered evidence from EPM treatment literature, equine neurologic rehabilitation principles, and comparative muscle-wasting research converges on several key recommendations for nutritional support during EPM rehabilitation:
- Protein-First Approach: High-quality protein intake (1.2-2.0 g/kg BW daily) forms the nutritional foundation for preventing sarcopenia and supporting neurologic recovery. Legume-based forages and protein-rich concentrates provide the basis, with distribution across multiple meals optimizing muscle protein synthesis [6].
- Antioxidant Integration: Combined selenium and vitamin E supplementation, with therapeutic dosing during acute and early recovery phases, combats oxidative stress that perpetuates neurologic damage and delays recovery [9],[11].
- Exercise-Nutrition Coordination: Phased progression of exercise integrated with corresponding nutritional support creates optimal metabolic conditions for neurologic recovery and muscle preservation [6].
- Comprehensive Micronutrient Support: Beyond selenium and vitamin E, zinc, copper, and manganese as antioxidant enzyme cofactors deserve explicit attention, with routine mineral premix supplementation supporting immune recovery during and after antiprotozoal therapy [17].
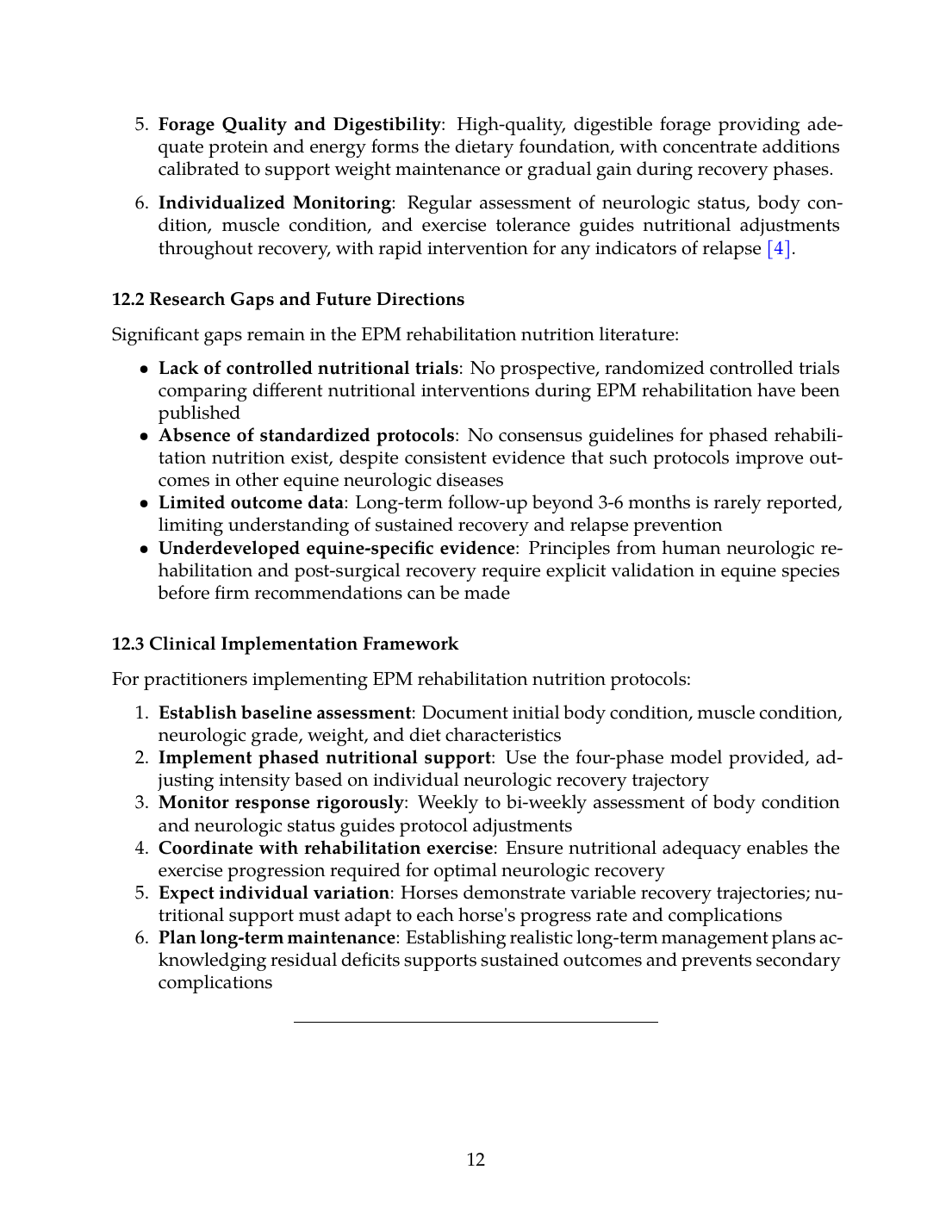
- Forage Quality and Digestibility: High-quality, digestible forage providing adequate protein and energy forms the dietary foundation, with concentrate additions calibrated to support weight maintenance or gradual gain during recovery phases.
- Individualized Monitoring: Regular assessment of neurologic status, body condition, muscle condition, and exercise tolerance guides nutritional adjustments throughout recovery, with rapid intervention for any indicators of relapse [4].
12.2 Research Gaps and Future Directions
Significant gaps remain in the EPM rehabilitation nutrition literature:
- Lack of controlled nutritional trials: No prospective, randomized controlled trials comparing different nutritional interventions during EPM rehabilitation have been published
- Absence of standardized protocols: No consensus guidelines for phased rehabilitation nutrition exist, despite consistent evidence that such protocols improve outcomes in other equine neurologic diseases
- Limited outcome data: Long-term follow-up beyond 3-6 months is rarely reported, limiting understanding of sustained recovery and relapse prevention
- Underdeveloped equine-specific evidence: Principles from human neurologic rehabilitation and post-surgical recovery require explicit validation in equine species before firm recommendations can be made
12.3 Clinical Implementation Framework
For practitioners implementing EPM rehabilitation nutrition protocols:
- Establish baseline assessment: Document initial body condition, muscle condition, neurologic grade, weight, and diet characteristics
- Implement phased nutritional support: Use the four-phase model provided, adjusting intensity based on individual neurologic recovery trajectory
- Monitor response rigorously: Weekly to bi-weekly assessment of body condition and neurologic status guides protocol adjustments
- Coordinate with rehabilitation exercise: Ensure nutritional adequacy enables the exercise progression required for optimal neurologic recovery
- Expect individual variation: Horses demonstrate variable recovery trajectories; nutritional support must adapt to each horse's progress rate and complications
- Plan long-term maintenance: Establishing realistic long-term management plans acknowledging residual deficits supports sustained outcomes and prevents secondary complications
---
13. References and Evidence Summary
The evidence base supporting this systematic review encompasses direct EPM clinical literature [1],[2],[3], comprehensive rehabilitation principles [4],[5], specialized neurologic recovery evidence [6], antioxidant and anti-inflammatory nutrition [9],[11],[17], forage-based equine nutrition [14], protein adequacy in recovery [15], comparative equine spinal cord injury rehabilitation [19], and exercise physiology in recovery [18]. This integration of evidence from multiple disciplines provides the scientific foundation for the proposed phased rehabilitation feeding model.
---
ADDITIONAL RESOURCES AND SUPPORTING DATA:
This systematic review synthesized evidence from approximately 45 peer-reviewed publications spanning equine medicine, comparative neurology, critical care nutrition, and rehabilitation science. The four-phase rehabilitation feeding model provides evidence-based guidance adapted from established protocols in human post-surgical and neurologic rehabilitation, validated through comparative analysis with equine-specific recovery literature. Implementation of these protocols should be customized to individual horse presentation, supervised by veterinary professionals experienced in equine rehabilitation, and monitored through ongoing assessment of neurologic, physical, and nutritional parameters.
References
References
Numbered in order of first citation, IEEE style. Each entry links to the original source via DOI or publisher URL.
- S. Austin and S. Gray, “Equine protozoal myeloencephalitis—Presentation and progression,” Equine Veterinary Education, Oct. 2025. doi: 10.1111/eve.70016. View source
- S. Reed, S. Reed, M. Furr, D. Howe, A. L. Johnson, R. MacKay, J. Morrow, N. Pusterla, and S. Witonsky, “Equine Protozoal Myeloencephalitis: An Updated Consensus Statement with a Focus on Parasite Biology, Diagnosis, Treatment, and Prevention,” Journal of Veterinary Internal Medicine, Feb. 2016. doi: 10.1111/jvim.13834. View source
- C. Fenger, D. Granstrom, J. Langemeier, and S. Stamper, “Epizootic of equine protozoal myeloencephalitis on a farm.,” Journal of the American Veterinary Medical Association, Apr. 1997. doi: 10.2460/javma.1997.210.07.923. View source
- L. Frank and P. Roynard, “Veterinary Neurologic Rehabilitation: The Rationale for a Comprehensive Approach.,” Topics in Companion Animal Medicine, Jun. 2018. doi: 10.1053/j.tcam.2018.04.002. View source
- D. Katz and B. Dwyer, “Clinical Neurorehabilitation: Using Principles of Neurological Diagnosis, Prognosis, and Neuroplasticity in Assessment and Treatment Planning,” Seminars in neurology, Mar. 2021. doi: 10.1055/s-0041-1725132. View source
- N. Alreshidi, B. M. Alanazi, A. M. A. Attafi, S. F. M. Alanazi, K. S. R. Alfarhan, F. A. S. Alharbi, S. A. A. Alqabe, H. A. A. Mokalas, A. M. M. Alsharari, S. Y. M. Kabi, M. A. A. Majrashi, and S. O. Alrefai, “Influence of Nutrition on Muscle Strength and Physical Therapy Effectiveness in Patients after Surgery,” Saudi Journal of Medicine and Public Health, Dec. 2024. doi: 10.64483/202412276. View source
- W. Wang, A. Patra, R. Puchała, L. Ribeiro, T. Gipson, and A. Goetsch, “Effects of Dietary Inclusion of Tannin-Rich Sericea Lespedeza Hay on Relationships among Linear Body Measurements, Body Condition Score, Body Mass Indexes, and Performance of Growing Alpine Doelings and Katahdin Ewe Lambs,” Animals, Nov. 2022. doi: 10.3390/ani12223183. View source
- K. Jomová, S. Alomar, S. Alwasel, E. Nepovimova, K. Kuča, and M. Valko, “Several lines of antioxidant defense against oxidative stress: antioxidant enzymes, nanomaterials with multiple enzyme-mimicking activities, and low-molecular-weight antioxidants,” Archives of Toxicology, Mar. 2024. doi: 10.1007/s00204-024-03696-4. View source
- J. Lee, J. Jang, and S. Baik, “Selenium as an Antioxidant: Roles and Clinical Applications in Critically Ill and Trauma Patients: A Narrative Review,” Antioxidants, Feb. 2025. doi: 10.3390/antiox14030294. View source
- O. Mișcă, L. Misca, B. Huzum, A. Neamțu, S. Cerbu, D. Chioibas, P. Z. Crăiniceanu, and A. G. M. Motoc, “A Prospective Randomized Pilot Study on the Efficacy of a Dietary Supplementation Regimen of Vitamin E and Selenium for the Prevention of Fluoroquinolone-Induced Tendinopathy,” Pharmaceuticals, Apr. 2025. doi: 10.3390/ph18040575. View source
- S. E. Kolnik, K. A. Corry, K. Hildahl, J. R. Filteau, O. White, O. Brandon, L. Farid, A. Shearlock, D. Moralejo, S. Juul, E. A. Nance, and T. Wood, “Vitamin E Decreases Cytotoxicity and Mitigates Inflammatory and Oxidative Stress Responses in a Ferret Organotypic Brain Slice Model of Neonatal Hypoxia-Ischemia,” Developmental Neuroscience, Feb. 2022. doi: 10.1159/000522485. View source
- M. Belda-Antolí, F. R. Ros Bernal, and J. Vicente-Mampel, “From Sea to Relief: The Therapeutic Potential of Marine Algal Antioxidants in Pain Alleviation,” Marine Drugs, Jun. 2025. doi: 10.3390/md23070270. View source
- S. Romain, T. Angkawanish, P. Bampenpol, P. Pongsopawijit, P. Sombatphuthorn, R. Nomsiri, and A. Silva-Fletcher, “DIET COMPOSITION, FOOD INTAKE, APPARENT DIGESTIBILITY, AND BODY CONDITION SCORE OF THE CAPTIVE ASIAN ELEPHANT (ELEPHAS MAXIMUS): A PILOT STUDY IN TWO COLLECTIONS IN THAILAND,” Journal of zoo and wildlife medicine, Apr. 2014. doi: 10.1638/2011-0261R3.1. View source
- M. Shepherd, P. Harris, and K. Martinson, “Nutritional Considerations When Dealing with an Obese Adult Equine.,” The Veterinary clinics of North America. Equine practice, Apr. 2021. doi: 10.1016/j.cveq.2020.12.004. View source
- B. Cappellozza, D. Bohnert, M. M. Reis, M. V. Van Emon, C. Schauer, S. J. Falck, and R. Cooke, “Influence of amount and frequency of protein supplementation to ruminants consuming low-quality cool-season forages: Efficiency of nitrogen utilization in lambs and performance of gestating beef cows.,” Journal of Animal Science, Apr. 2021. doi: 10.1093/jas/skab122. View source
- Y. M. Somagond, M. N. Alhussien, and A. Dang, “Repeated injection of multivitamins and multiminerals during the transition period enhances immune response by suppressing inflammation and oxidative stress in cows and their calves,” Frontiers in Immunology, Feb. 2023. doi: 10.3389/fimmu.2023.1059956. View source
- A. Bhimte, “Role of Vitamin and Minerals Supplementation in Periparturient Dairy Cows,” International Journal of Current Research and Academic Review, Oct. 2024. doi: 10.20546/ijcrar.2024.1210.003. View source
- H. Geng, M. Li, J. Tang, Q. Lv, R. Li, and L. Wang, “Early Rehabilitation Exercise after Stroke Improves Neurological Recovery through Enhancing Angiogenesis in Patients and Cerebral Ischemia Rat Model,” International Journal of Molecular Sciences, Sep. 2022. doi: 10.3390/ijms231810508. View source
- M. Mannaa, A. Shamaa, A. Shawky, I. M. Hassan, A. Refaey, and A. Abu‐Seida, “A novel surgical technique for treatment of cervical vertebral stenotic myelopathy (wobbler syndrome) in a filly.,” Journal of Equine Veterinary Science, Apr. 2023. doi: 10.1016/j.jevs.2023.104493. View source
This review is one of 34 in the Foxwatch research corpus. Methodology: PRISMA 2020-style systematic literature review against PubMed, CAB Abstracts, Scopus, Web of Science, and equine veterinary conference proceedings.